
New Interpretation of Galileo’s Arthritis and Blindness
Vol.05No.01(2015), Article ID:53899,10 pages
10.4236/aa.2015.51005
Alberto Zanatta1*, Fabio Zampieri1*, Maurizio Rippa Bonati1, Guido Liessi2, Cesare Barbieri3, Scott Bolton4, Cristina Basso1, Gaetano Thiene1#
1Department of Cardiac, Thoracic and Vascular Sciences, University of Padua Medical School, Padua, Italy
2C.M.S.R. Veneto Medica, Vicenza, Italy
3Department of Physics and Astronomy, University of Padua, Padua, Italy
4Space Science and Engineering Division, Southwest Research Institute (SwRI), San Antonio, USA
Email: #gaetano.thiene@unipd.it
Copyright © 2015 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/



Received 16 January 2015; accepted 4 February 2015; published 10 February 2015
ABSTRACT
Galileo Galilei (1564-1642) complained of several disorders during his life, the most important of which were chronic arthritic pains and bilateral blindness. These symptoms might be results from an immune rheumatic disease, namely reactive arthritis (urethritis, uveitis, arthritis), when Gali- leo started suffering with an episode of fever in June 1593. Padua University owns the fifth lumbar vertebra of the great scientist and we performed a series of anthropological and radiographic analyses on it. The anthropological measurements showed that the shape of the vertebra was normal as to exclude significant diseases. The study through radiography and Computed Tomography showed only a mild arthrosis documented by small osteophytosis. Eventually the disease evolved into blindness with a pannus restricting the pupils (uveitis). These findings support the occurrence of reactive arthritis. Alternatively to urethral infection, Galileo could have suffered from Chlamydia pneumoniae infection in 1593, which was complicated by reactive arthritis a couple of weeks later. Thereafter he complained several episodes of recurrent arthritis, which eventually culminated into uveitis and bilateral blindness.
Keywords:
Anthropology, Arthrosis, Galileo Galilei, Paleoanthropology, Reactive Arthritis

1. Introduction
Galileo Galilei (1564-1642) suffered during his life of several diseases. His clinical history, as it turns out from hundred letters he wrote and received, is so informative as to make it possible to delineate the natural history of his body (Favaro, 1966; Del Lungo & Favaro, 1968; Galilei, 1890-1909) . He complained about disorders related to rheumatism, kidney stones, haemorrhoids, inguinal hernia, arrhythmias, insomnia and melancholy. Moreover, he suffered from recurrent episodes of tertian fever (terzana).
Among all these disorders, chronic arthritic pains were the most constant in life and culminated into bilateral blindness. In this paper, we will advance a new diagnostic hypothesis of a correlation between these two diseases.
When Galileo died, his remains were temporarily buried in Florence’s Basilica of Santa Croce, in a room alongside the “Chapel of Cosma and Damiano”. The remains were not placed in the family vault, which was in the same church, because of Galileo’s heresy trial. One century later, in 1737, Galileo’s remains were exhumed to be finally placed in a Mausoleum in Santa Croce especially built for him. During this procedure, attracted by the idea to keep a “relic” from the great scientist, the priest Giovanni Vincenzo Capponi (1691-1748) took Galileo’s forefinger and thumb from the right hand, the man of letters Anton Francesco Gori (1691-1757) took the left hand forefinger, and the physician Antonio Cocchi (1695-1758) took the fifth lumbar vertebra.
Through several transfers, Galileo’s fifth lumbar vertebra was finally donated to the University of Padua by Domenico Thiene (1767-1844) on August 2nd 1823 (Zampieri et al., 2013) . The Rector of Padua University, Antonio Meneghelli (1765-1844), verified by a calligraphic investigation that the handwriting of the scroll attached to the vertebra (Figure 1) was originally made by its first holder, Antonio Cocchi, where was written:
Fifth lumbar vertebra taken from the body of the Great Galileo in the year of his exhumation and final entombment.
Rector Meneghelli got to do a “reliquary” for the vertebra, still preserved in the “Science Hall” of the Padua University “Palazzo Bo”, which consists of a wooden structure decorated with a Latin inscription:
I am the fifth lumbar vertebra and I permitted the flexion of the back of Galileo Galilei, who taught the new philosophy at this great University; Domenico Thiene from Vicenza gave me for an ornament of this Museum; Antonio Meneghelli, Rector Magnificus of this great University, attended to my being placed among his instruments in 1823.

Figure 1. Galileo’s fifth lumbar vertebra in his showcase with the original scroll (on the left). Close up of the Galileo fifth lumbar vertebra (on the right).
Considering “Galileo as a patient” (Thiene & Basso, 2011) , we will try a pathological anamnesis and a differential diagnosis based on historical letters and documents on Galileo’s health. Our hypothesis will be also supported by an anthropological analysis and Computed Tomography (CT) of Galileo’s fifth lumbar vertebra preserved at Padua University.
2. Material and Methods
We have consulted Galileo’s large correspondence and historical documents. Given the historical reports of Galileo’s symptoms and our hypothesis that he might have suffered from reactive arthritis, a study of his vertebra could yield new insight into the pathologies that affected him during his life. We describe a series of osteological measurements (Table 1) and results from a CT scan made on Galileo’s vertebra.
The osteological measurements were made following protocols from the “Laboratory of human paleontology” of the French National Centre of Research (CNRS) (Mafart, 1983) . We performed the following series of measurements: the Sagittal index, the Frontal index and the index of transversal enlargement (Table 1). We have measured, on the sagittal plane, the anterior and posterior heights from the borders of vertebral plates (Martin & Knuβmann, 1988) . The “sagittal index” is calculated as follows: (anterior height/posterior height) × 100. A sagittal non pathological index goes from a minimum of 104.0 to a maximum of 133.3 (Figure 2). Then we took the height of the vertebral body on the frontal plane passing through the centre of the antero-posterior diameter of the vertebral plates (for the thoracolumbar segment of the spine). The “frontal index” is given by the following formula: (left height/right height × 100). This formula indicates the inclination of the vertebral plates (Figure 3) (Mafart, 1983) . A normal spinal column has a frontal curvature centered on the axis 100 with minimal variations. The harmony of the curve is important because, even with small differences, a regular alternation of these signs on both the sides of the axis has a pathological significance. The study conducted by Mafart in the “Laboratory of human paleontology” finds a mean frontal index of 97.42 in individual judged as normal. The vertebral bodies are modified in their general shape as a consequence of osteoporosis, primary or secondary, which doesn’t permit a satisfying resistance to mechanical solicitations. These modifications give to the vertebral bodies a classic shape of hourglass with the enlargement of inferior and superior planes and a reduction in height. The “index of transversal enlargement” is given by the calculation: [(transversal superior diameter + transversal inferior diameter)/2 × (middle transversal diameter)] × 100 (Figure 3). According to Mafart, this index is rarely equal to 100, because of the marginal crest, and the value increases little by little from T1 to L5. Lumbar indexes less than 130 are considered.
We made also analysis using CT and digital radiography. The imaging was obtained by using digital Polidiagnost (Philips Healthcare) and a 64-channel CT scanner (Optima; GE Healthcare). The images were stored on a workstation Advantage 4.6 (GE Healthcare) for Multiplanar (MPR) and Virtual Reality (VR) reconstructions.
3. Results
Galileo’s vertebra absolute measurements are reported in Table 1. The sagittal index of the Galileo’s vertebra made on the mean values of the measurement is 126.17, a measure that is considered normal. The “frontal index” obtained on Galileo’s vertebra is 97.43, a value perfectly in line with the rate judged as normal. Galileo’s vertebra index of transversal enlargement is 112.30, another value considered normal.

Table 1. Galileo’s vertebra measurements (in millimetres). A, B, C are three different measurements taken at the same level to avoid intraobserver mistakes.
Values are given in millimetres.

Figure 2. The “sagittal index” is calculated as follows: (anterior height/posterior height) × 100; when the two vertebral plates are perfectly parallels, the ratio between anterior and posterior heights is 100.

Figure 3. The “frontal index” is given by: (left height/right height) × 100 (on the left); the “index of transversal enlargement” is given by: [(transversal superior diameter + transversal inferior diameter)/2 × (middle transversal diameter)] × 100 (on the right).
From an anthropological point of view, in conclusion, Galileo’s vertebra has a normal shape with no evidence of pathological processes.
On CT and digital radiography (Figure 4 and Figure 5), the thickness of the cortical bone ranged between 1 to 2 mm. The spongy bone was well delineated but near the pedicle some symmetric sharp lytic foci probably due to bony vessels were present. The thickness of cortical bone of laminae, trasverse, articular and spinous process
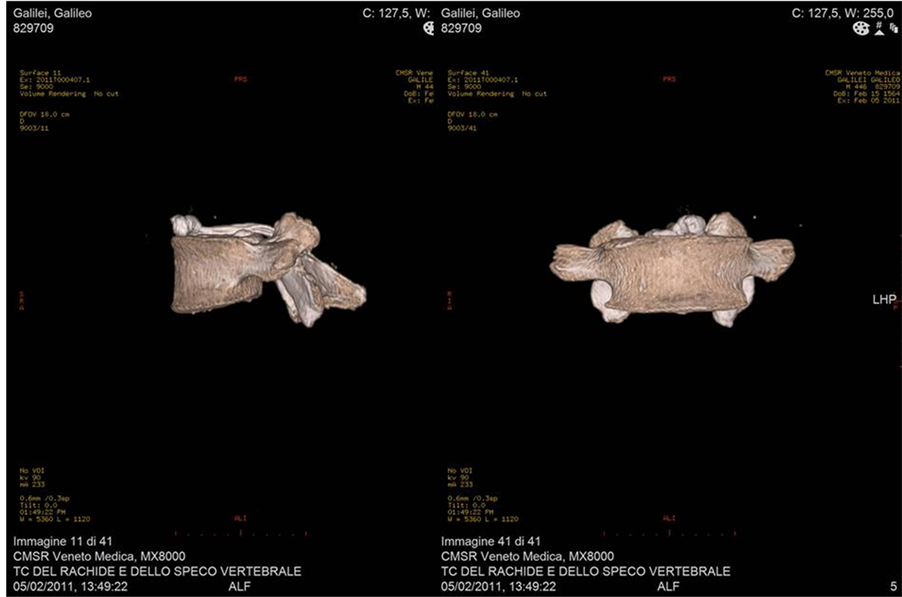
Figure 4. TC of the vertebra. On the left it is appreciable the anterior height of the vertebral plate higher than the posterior; on the right it is appreciable the light inclination of vertebral plates.

Figure 5. Radiography of the vertebra from the superior face (left); TC of the vertebra from the superior face (right).
varies from 1 mm in trasverse process to 3.2 mm in articular process and laminae. Also the cancellous bone of the vertebral arch elements shows vascular spaces. The contours of the trasverse process were irregular with small notches of osseous matter. The edges of body show small osteophytes more evident at the contour of the superior endplate. Mild osteoarthrosis was visible also for superior and inferior articular process, mostly the superior. The contours of vertebral canal were regular without lysis or notches of cortical bone; the canal showed a triangular shape and the anteror-posterior diameter was 16.9 mm and the latero-lateral one 32.4 mm.
4. Discussion
Galileo’s life-style was a bit libertine, since he was a great eater, drinker and sexually very active. Until middle age, he was said to be of cheerful and pleasant countenance, square of frame, well-proportioned and above middle height. His complexion was fair and sanguine, his eyes blue and sparkling and his hair and beard (of which he had in abundance) of a reddish hue (Favaro, 1966; Thiene & Basso, 2009) .
The first disorder affecting Galileo was an episode of “serious opthalmia” in 1579, as reported by the friar Diego Franchi da Genova (?-1652), when he was novice at the Vallombrosa abbey (Galilei, 1890-1909; Grondona, 1967) . It was probably a simple stye, but reason enough for Galileo’s father to take the child home and keep him far from the monastic carrier (Viviani, 1654; Favaro, 1966) .
A very severe illness, which Galileo himself linked to the subsequent morbid manifestations, occurred in the early summer of 1593, when he was 29 years old and spent a weekend in a villa of Costoza near Vicenza of Count Camillo Trento (Favaro, 1966) . During a hot day in June, after a hearty meal and wine drinking with friends, Galileo and the others fellows slept in the so called “Sala dei Venti” (Wind Room) (Figure 6), a room which was constantly cooled by air, circulated through large ventiducts from the nearby caves. They woke up severely ill with high fever, cramps, chills, haemorrhages, intense headaches, and lethargy. One of them died in a few days, another died in three weeks after losing his hearing, and Galileo, who survived, remained deaf for one year.
From that occasion Galileo started to complain chronic arthritic pains. His disciple and biographer Vincenzo Viviani (1622-1703) reported the episode as follows:

Figure 6. Entry of the “Wind Room” in the villa of the Count Camillo Trento where Galileo and his two friends slept during a summer weekend, June 1593.
[…] acute pains and punctures which bother him in different parts of the body during changes of weather, originated from his stay, with two nobles of his friends, during a very hot summer in a Padua countryside Villa, when they slept in un a room very cold to escape the boring hours of the day […] here a servant inadvertently opened a window through which cooled a perpetual artificial wind generated by the movements of waters nearby flowing. This wind, being too much humid and cold, finding their bodies without clothes during the two hours in which they slept, introduced in them so much worst quality that, when they woke up, all were severely sick and one died in few days, another lost hearing and didn’t lived so long, and Galileo suffered from the above-mentioned indisposition from which he never recovered (Viviani, 1654) .
The recurrence of arthritis in Galileo’s life is confirmed by his son Vincenzio Galilei (1606-1649), who told Viviani that his father was afflicted all lifelong by “arthritic pains” (Favaro, 1966) .
In December 1606, when returning to Florence at the Medicean Villa in Pratolino for the education of the adolescent Cosimo de’ Medici (1590-1621), Galileo suffered from an attach of tertian fever, which was successfully cured by Tommaso Minadoi (1549-1615) and Girolamo Fabrici d’Acquapendente (1537-1619), famous anatomist. In a letter to Cristina di Lorena (1565-1637), Grand Duchess of Tuscany and mother of Cosimo, dated December 8th 1606, Galileo wrote:
The disease started the night before the departure from Pratolino and hold me ailing for eight days in Florence. When it leaved me enough strength to move to Padua, breaking the ceasefire two days after my arrival here, stopped me at bed such as a tertian. After changing in continuous fever, still retains me ill (Galilei, 1890-1909; Del Lungo & Favaro, 1968) .
From 1608 to 1610 Galileo had relapsing episodes of fever, which in a letter dated March 19th 1610 he attributed to having “spent most of the night time in the winter more in the open space than in the bedroom or at the fireplace” with the telescope (Favaro, 1966) . On December 1611 he suffered from articular pains, “blood profusion” (probably from haemorrhoids) and “lethargy of stomach” (Galilei, 1890-1909) . On May 1612 again “limb pains and fever”, other than sleeplessness and inappetence (Galilei, 1890-1909) . On January 1613 he suffered of a renal colic generating sandy stones (Galilei, 1890-1909) .
The first reliable episode of sight failure is reported in chapter 49 of his Il Saggiatore, where he mentioned a corneal halo which occurred in 1616 (Galilei, 1890-1909; Watson, 2009) . In 1617 he complained “the return of my usual pains” because of arthritis, increasing inguinal hernia and piles (Galilei, 1890-1909) . On November 1618, he informed the friends to be forced to bed “due to longstanding and dangerous illness” (Galilei, 1890-1909) . In the spring of 1629 he claimed to have suffered from a transient loss of hearing so severe to be “unable to hear an artillery” (Thiene & Basso, 2011) .
Galileo presented a fluxion from the right eye in 1624. By checking his portrait made by Ottavio Leoni (1568-1630), painted exactly in 1624, you can easily see right supraorbital swelling and wrinkling consistent with frontal sinus mucocele (Figure 7). On December 17th 1631 he had a “fluxion” (“sciesa”) on both eyes, which hindered him to read and write for two months (Di Fernando, 1994) .
In 1632, following his reluctance, due to alleged sickness, to obey the Pope Urbano VIII (1568-1644) to move to Rome and be inquired by the Holy Office for the Dialogue affair, he underwent to a “medical” check of his health conditions by three eminent physicians committed by the same Urbano VIII (Secchi, 1868) . They recorded:
His pulse intermits every three or four beats, from which we conclude that his vital powers are affected, and at his great age much weakened. To the above are to be ascribed frequent attacks of giddiness, hypochondriacal melancholy, sleeplessness and flying pains about the body to which other can testify […]. We have also observed serious hernia with rupture into the peritoneum. All these symptoms are worthy of notice, as under the least aggravation they might become harmful to life (Viviani, 1654) .
He very likely had atrial fibrillation or incomplete atrio-ventricular block (Thiene & Basso, 2011) . It is interesting to note that in this medical report there is no mention of ocular problems at all.
On April 27th 1634, Galileo stated “My health condition is in trouble. The hernia increase more than ever, the pulse is intermittent with palpitations, I feel odious to myself with immense sadness and extreme inappetence” (Galilei, 1890-1909) .
Galileo had a fluxion from the right eye on February 1636. We have found another notice on a mild complaint

Figure 7. Ottavio Leoni, Portrait of Galileo, 1624, engraving, Istituto Nazionale per la Grafica, Rome. Note the right supraorbital swelling and wrinkling, in keeping with mucocele.
on the right eye on February 11th 1637 (Galilei, 1890-1909; Grondona, 1967) , while on July 4th he completely lost the vision on this eye, as reported in a letter to Élie Diodati (1576-1661), Swiss lawyer and jurist (Galilei, 1890-1909) . On November 5th of the same year the left eye started to be affected, “also it launched […] toward obscurity” (Galilei, 1890-1909) . At Christmas he was bilaterally blind, because he was unable to see anything “apertis oculis quam occlusis” (with the eyes either open or closed) (Galilei, 1890-1909) .
A famous passage is in a letter to Élie Diodati, written by Galileo on January 2nd 1638:
[…] Galileo, your beloved friend and servant, has been irreparably blind for one month. Consider you in what an affliction I find myself, while I’m thinking that this sky, this world and this universe that I expanded hundred and even thousand times more than commonly seen by the learned of the past with my wonderful observations and clear demonstrations, now for me it is so diminished and restricted that it is no more than the borders of my body (Galilei, 1890-1909) .
The blindness is demonstrated by the change of Galileo’s signature, from a clear and elegant to a very uncertain and undefined trait (Figure 8).
Regarding the blindness, there is a diagnosis, made at distance by letter, of the roman surgeon Giovanni Trullio (1598-1661). The written consultation of Trullio reports:

Figure 8. Change of Galileo’s signature from the normal eyesight (April 4th 1637) to the bilateral blindness (March 13th 1640, letter to Leopoldo de’ Medici [1617-1675]).
[…] blindness is due to a suffusion which obstructs the pupil and which is incorrectly defined as a cataract […] because the seat of the disease is not in the surface of the eyes, but in between the cornea and uveal tunica, at the base of which there is the aqueous humour […] this happening inside the eyes, which became progressively thicker and harder, can be decompressed by a needle with the help of God (Galilei, 1890- 1909 ).
Thanks to this document, we can exclude a senile cataract and interpret the blindness as the result of an uveitis with condensation of the aqueous humour and formation of a film restricting the pupils, which Trullio called “skin of pupil”. Trullio, due to the suspicion of ocular hypertension (glaucoma), suggested a needle decompression, if necessary.
To explain the progressive blindness of Galileo, different diagnoses have been postulated by scientists (Secchi, 1868; Gradenigo, 1898; Germani, 1964; Mancini, 1964; Grondona, 1967; Di Fernando, 1994; Watson, 2009) , as the origin of this disorder: actinic damage due to observations of sunspots through the telescope; ophthalmia during the novitiate at the Vallombrosa abbey; uveitis due to brucellosis got in Pratolino; uveitis from an immune rheumatic disorder.
What we can render unlikely, at any case, is uveitis in the course of brucellosis, because this infection leaves on the vertebrae typical signs of erosion which are completely absent in Galileo’s fifth lumbar vertebra (Mutolo et al., 2012) .
The hypothesis of uveitis from a rheumatic disorder is the most plausible because it explains the arthritic pains which deeply characterized Galileo’s life history. That the blindness of Galileo might be correlated with an autoimmune rheumatic disease has been the most frequent advanced hypothesis (Gradenigo, 1898; Germani, 1964; Grondona, 1967; Watson, 2009) , including Reiter syndrome, which is also referred as “reactive arthritis” (Watson, 2009) .
Reactive arthritis is characterized by the triad: conjunctivitis, urethritis and arthritis (Kvien et al., 1994; Wu & Schwartz, 2008) . There is an involvement of knees, ankles and more rarely spinal column (12% - 16%). It is an autoimmune disease, triggered or “reactive” to an infection, so to be called “reactive arthritis”. The trigger can be venereal diseases, such as Chlamydia trachomatis, or intestinal infections, in particular Salmonella, or respiratory infection, especially Chlamydia pneumoniae. The syndrome affects young males between 20 and 40 years old. The antigenic susceptibility is characterized by the fact that 80% of affected persons is HLA-B27 positive, versus 6% of the normal population.
A hypothesis might be that Galileo suffered from an undisclosed urethritis due to venereal infection. He complained of a “continuous kidneys pains” for two months (Galilei, 1890-1909) . In another letter dated January 1st 1614 he mentioned a burning sensation with urination, called by him “burning urine” (Galilei, 1890-1909) . Was this a symptom of urethritis? Concerning this possible infection, he could have been discreet, since urethritis is usually the consequence of sexual libertine intercourse, obviously deleterious for his reputation.
Reactive arthritis in Galileo might have been triggered by a Chlamydia pneumoniae infection taken during the febrile episode of the summer weekend in the villa near Padua, where he and his friends had an acute illness after a prolonged exposition to a cool wind. The symptoms described in the historical account are compatible with Chlamydia pneumoniae, because of fever, bronchitis (even fatal), pharyngitis, sinusitis, otitis and myocarditis (Grayston et al., 1990) . They are, at the same time, less compatible with a Salmonella infection, because Galileo and his friends did not complain abdominal pains, nausea or vomit after the meal. Although the infection by Chlamydia pneumoniae is fatal only in the presence of pre-existing morbid conditions, the deafness of Galileo and friend is in keeping with otitis which is frequently associated with Chlamydia pneumoniae infection.
Galileo started to complain arthritic pains just after this episode, suggesting that the reactive arthritis could have been triggered by the infection of Chlamydia pneumoniae, considering also that this syndrome is more frequent in young males between 20 and 40 years old (Galileo was 29 years old at that time) (Braun et al., 1994; Hannu et al., 1999) . Reactive arthritis eventually could have caused uveitis which lead Galileo to bilateral blind- ness.
Reactive arthritis is an auto-immune inflammation which involves the synovial tissue of affected joints and it is not associated with bone erosions. The anthropological measurements of the fifth lumbar vertebra of Galileo show that its shape has nothing that could be considered as the result of severe pathological process. Moreover, radiography and CT studies, showed only a mild arthrosis documented by a minimal osteophytosis. However, the negative findings at the examination of Galileo fifth lumbar vertebra by no means exclude the occurrence of reactive arthritis. Large joints of the lower limbs are usually affected, whereas spondiloarthritis rarely occurs. Among the several symptoms, Galileo never complained back pain in his life. This is confirmed by the fact that, when Galileo was sick, he passed long time at bed, as reported in his letter. As well known, those who suffer of back pains cannot stay long stretched out, because this position exacerbates the painful sensation. Thus, it is not surprising that Galileo’s lumbar vertebra bone appears almost intact.
5. Conclusion
In conclusion, alternatively to urethral infection, suspicion of which arises from some letters, we may postulate that Galileo had a Chlamydia pneumoniae infection at the Wind Room in Costozza in 1593, which was complicated by reactive arthritis a couple of weeks later. Acute reactive arthritis may evolve into a chronic arthritis, as it occurred in Galileo. Thereafter he suffered several episodes of recurrent arthritis, which eventually evolved into uveitis and bilateral blindness.
Conflict of Interest Statement
We declare that we have no conflict of interest.
References
- Braun , J., Laitko, S., Treharne, J., Eggens, U., Wu, P., Distler, A., & Sieper, J. (1994). Chlamydia Pneumoniae―A New Causative Agent of Reactive Arthritis and Undifferentiated Oligoarthritis. Annals of the Rheumatic Diseases, 53, 100-105. http://dx.doi.org/10.1136/ard.53.2.100
- Del Lungo, I., & Favaro, A. (Eds.) (1968). Dal carteggio e dai documenti: Pagine di vita di Galileo. Firenze: Sansoni.
- Di Fernando, R. (1994). Il Linceo cieco. In: Idem 1994, Fiaccole spente alla festa delle capanne: Saggi di storia oftalmologica (pp. 127-150). Pesaro: Nobili.
- Favaro, A. (1966). Galileo Galilei e lo Studio di Padova, 2 vols. Padova: Antenore.
- Galilei, G. (1890-1909). Le opere di Galileo Galilei: Edizione nazionale sotto gli auspici di Sua Maestà il Re d’Italia, 20 volumi. Firenze: Barbéra Editore.
- Germani , G. M. (1964). Malattia reumatoide e cecità di Galileo Galilei. Ospedale Maggiore LIX, 2, 193-196.
- Gradenigo, P. (1898). La malattia che determinò la cecità di Galileo Galilei. Venezia: Tipografia Ferrari.
- Grayston, J. T., Campbell, L. A., Kuo, C. C., Mordhorst, C. H., Saikku, P., Thorn, D. H., & Wang, S. P. (1990). A New Respiratory Tract Pathogen: Chlamydia pneumoniae Strain TWAR. Journal of Infectious Disease, 161, 618-625. http://dx.doi.org/10.1093/infdis/161.4.618
- Grondona, F. (1967). In tema di eziogenesi della cecità di Galileo. In: Atti del simposio internazionale di storia, metodologia, logica e filosofia della scienza Galileo nella storia e nella filosofia della scienza (Firenze-Pisa, 14-16 September 1964) (pp. 141-154). Firenze: Barbéra Editore.
- Hannu, T., Puolakkainen, M., & Leirisalo-Repo, M. (1999). Chlamydia Pneumoniae as a Triggering Infection in Reactive Arthritis. Rheumatology, 38, 411-414. http://dx.doi.org/10.1093/rheumatology/38.5.411
- Kvien, T., Glennås, A., Melby, K., Granfors, K., Andrup, O., Karstensen, B., & Thoen, J. (1994). Reactive Arthritis: Incidence, Triggering Agents and Clinical Presentation. Journal of Rheumatology, 7, 188-192.
- Mafart, B. Y. (1983). Pathologie osseuse au Moyen Age en Provence (p. 52). Paris: Editions du Centre National de la Re- cherche Scientifique.
- Mancini, C. (1964). Le malattie di Galilei. In Atti del XX congresso nazionale di storia della medicina (pp. 284-294). Roma: Società Italiana di Storia della Medicina.
- Martin, R., & Knuβmann, R. (1988). Anthropologie. Handuch der vergleichenden Biologie des Menschen (p. 194). Stuttgart and New York: Gustav Fischer Verlag.
- Mutolo, M. J., Jenny, L. L., Buszek, A. R., Fenton, T. W., & Foran, D. R. (2012). Osteological and Molecular Identification of Brucellosis in Ancient Butrint, Albania. American Journal of Physical Anthropology, 147, 254-263. http://dx.doi.org/10.1002/ajpa.21643
- Secchi, P. A. (1868). Sull’epoca vera e la durata della cecità del Galileo. Giornale Arcadico di Scienze, Lettere ed Arti, LIV, 1-52.
- Thiene, G., & Basso, C. (2009). Atti e Memorie dell’Accademia Galileiana di Scienze Lettere ed Arti in Padova. I mali di Galileo, CXXI, II, 25-36.
- Thiene, G., & Basso, C. (2011). Galileo as a Patient. In E. M. Corsini (Ed.), The Inspiration of Astronomical Phenomena VI (pp. 73-83). Ann Arbor, MI: Sheridan Books.
- Viviani, V. (1654). Racconto istorico della vita di Galileo. In A. Favaro (Ed.), Edizione Nazionale delle opere di Galileo Galilei (pp. 609-610). Vol. XIX. Firenze: Barbéra Editore.
- Watson, P. G. (2009). The Enigma of Galileo’s Eyesight: Some Novel Observations on Galileo Galilei’s Vision and His Progression to Blindness. Survey of Ophthalmology, 54, 630-640. http://dx.doi.org/10.1016/j.survophthal.2009.03.002
- Wu, I. B., & Schwartz, R. A. (2008). Reiter’s Syndrome: The Classic Triad and More. Journal of the American Academy of Dermatology, 59, 113-121. http://dx.doi.org/10.1016/j.jaad.2008.02.047
- Zampieri, F., Zanatta, A., Rippa Bonati, M., & Thiene, G. (2013). Medizingeschichtliche Anmerkungen zum fünften Len- denwirbel Galileo Galileis in der Universität Padua. In A. Wieczorek, G. Rosendahl, & D. Lippi (Eds.), Die Medici. Menschen, Macht und Leidenschaft (pp. 352-355). Regensburg: Schnell und Steiner.
NOTES

*Equal contributors.
#Corresponding author.
上一篇:Mapping Three-Dimensional Dens 下一篇:The Major Y-Chromosome Haplogr
最新文章NEWS
- Soft Tissue Contributions to Pseudopathology of Ribs
- Genotoxicity Assessment of Birch-Bark Tar—A Most Versatile Prehistoric Adhesive
- Mapping Three-Dimensional Density Patterns for Analyzing Artefact (Re)distribution Trends in Palaeol
- Ancient History of the Arbins, Bearers of Haplogroup R1b, from Central Asia to Europe, 16,000 to 150
- Re-Examining the "Out of Africa" Theory and the Origin of Europeoids (Caucasoids) in Light
- The Origin of Kurds
- There Are <i>ponoks</i>, and There Are <i>ponoks</i>: Traditional Religious
- Extirpolation of the Mythology that Porotic Hyperostosis is Caused by Iron Deficiency Secondary to D
推荐期刊Tui Jian
- Chinese Journal of Integrative Medicine
- Journal of Genetics and Genomics
- Journal of Bionic Engineering
- Pedosphere
- Chinese Journal of Structural Chemistry
- Nuclear Science and Techniques
- 《传媒》
- 《中学生报》教研周刊
热点文章HOT
- The Ancient Egyptian Hieroglyphic Language Was Created by Sumerian Turks
- Integrating Biomarkers into Research with Latino Immigrants in the United States
- Analyses of Dermatoglyphic Patterns in Ntamante, Boki Local Government Area (LGA) of Cross River Sta
- Molecular Genetic Perspectives on the Origin of the Lyngngam Tribe of Meghalaya, India
- The Effect of Working Place on Worker’s Health in a Tannery in Bangladesh
- Future Options of the Kurds.1Part I: The Current Situation
- Genotoxicity Assessment of Birch-Bark Tar—A Most Versatile Prehistoric Adhesive
- Could Wading in Shallow Water Account for the Unique Shape of the Australopithecus afarensis Pelvis?