
The Current Treatment and Prevention of Post Herpetic Neuralgia
Vol.02No.01(2018), Article ID:83322,11 pages
10.4236/ym.2018.21003
Simant Ankit1, Tongxiang Zeng1*, Yangxin Chen1, Hari Narayan Gupta2, Kunal Shah1, Xianwang Wang1,3*
1Department of Dermatology & Venereology, Jingzhou Central Hospital & The Second Clinical School of Medicine, Yangtze University, Jingzhou, China
2Department of Dermatology & Venereology, Tribhuvan University, Kathmandu, Nepal
3Laboratory of Oncology, Center for Molecular Medicine, School of Medicine, Yangtze University, Jingzhou, China

Copyright © 2018 by authors and Scientific Research Publishing Inc.
This work is licensed under the Creative Commons Attribution International License (CC BY 4.0).
http://creativecommons.org/licenses/by/4.0/



Received: December 12, 2017; Accepted: March 24, 2018; Published: March 27, 2018
ABSTRACT
Post herpetic neuralgia (PHN) is a chronic neuropathic pain syndrome in the area of the herpes zoster (HZ) rash, persisting after the cutaneous lesions have subsided. Despite numerous treatment advances, many patients remain refractory to the current therapies and continue to have pain, physical, economical and psychological distress. In this review, we will focus on the current treatment and prevention of PHN.
Keywords:
Post Herpetic Neuralgia, Current Treatment, Prevention

1. Introduction
Herpes zoster (also known as Shingles derived from Latin word “cingulum” meaning belt) is defined as a neurocutaneous disorder due to reactivation of the varicella zoster virus in craniospinal sensory neuron. It is an acute segmental eruption of herpetiform vesicles on the skin affecting the unilateral dermatomes and average age is between 50 - 65 years [1] . Dermatomal distributions are thoracic 53%, cervical 20%, trigeminal including ophthalmic 15%, lumbosacral 11% and bilateral involvement is rare [2] . The characteristic zoster pain is often accompanied by substantial pain, dysesthesia (abnormal sensation) and skin eruption. In many patients pain resolves once the affected area of the skin returns to normal. However, some patients continue to experience pain long after the lesions have healed. The pain is commonly called as post herpetic neuralgia (PHN), which is the most common complication of herpes zoster (HZ) [3] .
Although a variety of definitions of PHN have been used by clinicians, the most recent one is described in three levels [4] [5] , pain persist within 30 days from the onset of rash is defined as acute herpetic neuralgia; pain present between 30 and 120 days is defined as sub acute herpetic neuralgia; pain persisting after 120 days from the onset of HZ is defined as PHN. Post herpetic pain may take several forms, including allodynia (non painful stimulus perceived as painful), hyperpathia (slightly painful stimulus perceived as very painful), and dysesthesia (abnormal sensation with no stimuli).
It occurs in patients older than 80 years about in 30% of cases and in patients 60 to 65 year is 20% - 30% and it is rare in patients younger than 50 years. Women are at greater risk of PHN [6] . According to several studies the average annual incidence rate in different part of the world is Australia (9.67/1000) [7] , United States (8.46/1000) [8] , South Korea (10/1000) [9] and 9.65/1000 in China [10] . Despite numerous treatment advances, many patients remain refractory to the current therapies and continue to have pain, physical, economical and psychological distress. Here we focus on the current treatment and prevention of PHN.
2. Treatment of Post Herpetic Neuralgia
According to many research and evidences pain relief in PHN with currently available therapies is often complex and often need a multidisciplinary approach as shown in Table 1. Treatment is to control pain and wait for the condition to resolve. As shown in Figure 1, current guidelines recommend treatment of PHN with calcium channel α2-δ ligands (gabapentin and pregabalin), tricyclic antidepressants (amitriptyline, nortriptyline, or desipramine), or topical lidocain patches as first-line drugs; opioids and topical capsaicin patch or cream as second-line treatment options, or combination therapies with different mechanisms of action [11] [12] .
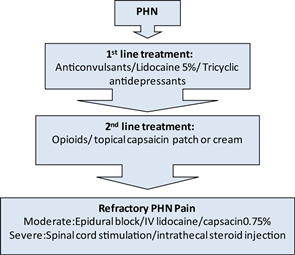
Figure 1. Overview of management strategies for the treatment of patients with post herpetic neuralgia (Abbreviation: PHN: post herpetic neuralgia, IV: intravenous).

Table 1. Management of postherpetic neuralgia.
2.1. Anticonvulsants
The anticonvulsants appear to be effective and drugs are gabapentin, pregabalin, phenytoin and carbamazepine. The anticonvulsants gabapentin and pregabalin bind to a two-dimensional protein, where they act as voltage-gated calcium channel blockers, inhibiting central pain pathways. Gabapentinoids (gabapentin and pregabalin) have been studied extensively for PHN. Their advantage is lack of pharmacokinetic interactions, as they are not bound to plasma proteins and are secreted to urine without hepatic metabolism. Gabapentin has a saturable transport mechanism in the gut, whereas absorption of pregabalin is more linear. There are several studied done to prove these drugs to be successfully recommended for the PHN by different researchers in different years such as Sabatowski on 2004 and van Seventer on 2006 on pregabalin with doses 150, 300 and 600 mg in number of pt (157/238) for 8 weeks and (281/370) for 13 weeks respectively. The result shows maximum number of patients is benefited in decreasing the pain. Similarly for gabapentin, Rowbothan on 1998 and Rice & Maton on 2001 with doses 3600 mg and 1800, 2400 mg in number of patients 229 and 334 respectively for 8 weeks and all cases outcome was positive to decrease the pain. Recently, two randomized controlled trials done on 2015 support the use of gabapentin to treat PHN. The dosage was started at 300 mg daily and titrated over two weeks to a maximum of 3600 mg daily. This study proves that using smaller doses 1800 mg daily was as effective and better tolerated than 2400 mg daily [13] . The most common adverse effects with gabapentin and pregabalin include somnolence (up to 25%) and dizziness (up to 46%). Carbamazepine acts by antagonizing sodium channels, stabilizing pre- and post-synaptic neuronal membranes. It is used for several diseases inducing neuropathic pain. It is very effective for paroxysmal and excruciating pain and less effective for burning pain and allodynia.
The New Drug Application (NDA) for DM-1796 drug was accepted by the US Food and Drug Administration (FDA) for the management of PHN. It is an extended release, formulation of gabapentin, once-daily tablet, which is designed to reduce the dosing frequency and have a low incidence of side effects. The NDA follows the completion of a randomized, double-blind, placebo controlled Phase 3 study of 452 PHN patients. The study concluded that 1800 mg of DM-1796 dosed once daily shows significant reduction in the pain associated with PHN. The most common side effects observed in patients receiving DM-1796 were dizziness and somnolence [14] . By Aestus Therapeutics ATx08-001 drug which is being tested, particularly for the pain associated with PHN. This drug is an orally-available Peroxisome Proliferator Activator Receptor [PPAR]-gamma agonist, which has been examined over 800 patients, has characteristically shown safety and better toxicology profile. The research on this drug is being directed to justify it as first-line treatment for neuropathic pain [15] .
2.2. Analgesic
2.2.1. Topical Agents
Recent studies done on 2014 by The FDA has approved two topical medications for treatment of PHN that include the topical lidocaine 5% patch (Lidoderm) as a first-line therapy, and the capsaicin 8% patch as a second-line therapy. Topical lidocaine acts by blocking sodium channels and decreasing abnormal ectopic discharges. Topical lidocaine patches are particularly effective for patients with allodynia (pain from stimuli which are not normally painful) [16] . There are only mild-to-moderate side effects such as pruritus, erythema and dermatitis. Capsaicin (trans-8-methyl-N-vanillyl-6-nonenamide) is a highly selective agonist for the transient receptor potential vanilloid 1 receptor (TRPV1). The initial effect of capsaicin is the activation of the TRPV1-expressing cutaneous nociceptors, which result in pungency (powerful odor or taste) and erythema due to the release of vasoactive neuropeptides. The capsaicin 8% patch has shown only minimal analgesic efficacy in patients with PHN. Side effects are erythema (most common), pain, pruritus, and papules [17] . Lotions containing calamine (e.g., Caladryl) may be used on open lesions to reduce pain and pruritus. Once the lesions have crusted over, capsaicin cream (Zostrix) may be applied [18] [19] .
2.2.2. Opioids
Opioid analgesic helps to reduce acute pain in patients with HZ because of their diverse mechanisms of action in the Central nervous system and Peripheral nervous system as well as their demonstrated efficacy in patients with both inflammatory and neuropathic pain including PHN [20] [21] [22] . Preliminary analyses of a recent randomized trial showed that controlled-release shown that patients taking oxycodone, morphine, or methadone have better pain relief than those taking placebo. Oxycodone is of special concern because of a 50 percent higher serum concentration when creatinine clearance is less than 60 mL per minute per 1.73 meter square (1.00 mL per second per meter square) [23] . Morphine and methadone have been shown to provide better pain relief than TCAs [24] . Tramadol, a weak m-opioid agonist that also inhibits the reuptake of nor epinephrine and serotonin, is efficacious in patients with PHN.
2.3. Tricyclic Antidepressants (TCAs)
TCAs can be effective in reducing the neuropathic pain of postherpetic neuralgia by inhibiting the reuptake of serotonin and nor epinephrine neurotransmitters. Drugs commonly used are amitriptyline, nortriptyline, imipramine and desipramine. Randomized, double-blind trials comparing two different treatments for patients with PHN have supported this fact that nortriptyline is equivalent in efficacy to amitriptyline, but is better tolerated [25] . These drugs are best tolerated when they are started in a low dosage and given at bedtime. The dosage is increased every two to four weeks to achieve an effective dose. Treatment with TCAs can occasionally lead to cardiac conduction abnormalities or liver toxicity. The potential for these problems should be considered in elderly patients and patients with cardiac or liver disease. Because TCAs do not act quickly, a clinical trial of at least three months is required to judge a patient’s response [26] . Some new antidepressants, such as, venlafaxine, bupropion, and paroxetine have analgesic properties have shown effective in PHN [15] , but there is not much evidence to support.
2.4. Interventional Treatment
Some patients with PHN may have persistent pain despite pharmacological, topical, psychological, and physical therapies. These cases of refractory PHN may be managed using epidural injections, paravertebral nerve blocks and sympathetic nerve blocks. In a randomized control trail (RCT) conducted in 2006, it was shown that a single epidural injection of 80 mg methylprednisolone acetate plus bupivacaine significantly reduced acute pain from HZ and helps in reducing the pain of PHN compared to intravenous administration of acyclovir and prednisolone [27] . Para vertebral block (PVB) produces unilateral segmental block with the spinal nerve dorsal ramus, and the sympathetic chain. PVB is easier with a favorable side effect profile, but has similar analgesic efficacy, compared to epidural block. In recent clinical trial (2015), it was found that PVB with local anesthetics plus steroids is effective for relief of acute herpetic pain and prevention of the incidence of PHN [28] [29] . Sympathetic nerve block is often used for HZ patients. In a RCT in 2012, early sympathetic nerve block for facial HZ, in combination with antiviral agents, was found to provide significant reduction of the severity and duration of pain and to decrease the incidence of the development of PHN [30] .
2.5. Ozone Therapy
HZ and PHN are normally treated with viral static agents as the preferred method. In comparison to viral static agents, ozone therapy also has shown good results. There are a number of scientific studies, reviews and papers documenting excellent results in the treatment of HZ and PHN with ozone therapy. Ozone disrupts the viral capsid and the viral reproductive cycle by interrupting the virus-to-cell contact with peroxidation and reducing the pain. According to a retrospective study of 55 cases of PHN done by Dr. Heinz Konrad, he concluded that ozone therapy when given 1000 microgram three times per week for 4 - 6 weeks make a significant pain reduction in PHN. Among 55 cases, pain reduction in 22 patients was 100%, 16 patients 75% and 7 patients no pain reduction [34] . Beside, in recent studies on animal models ozone has shown analgesic effect in neuropathic pain [35] .
As summarized in Table 1, there is several therapeutic management of pain in PHN patients. However, PHN is a complex condition, is difficult to treat, and requires a methodical therapeutic approach, and physician assistants and nurse practitioners are critical in coordinating team-based and patient-centered care. Thus, is particularly important.
3. Prevention of PHN
A primary varicella vaccine is a live attenuated varicella zoster vaccine (VZV) using the Oka/Merck strain. Vaccination given during the childhood period decreases the incidence of chickenpox, subsequent HZ reactivation, and acute herpes zoster (AHZ) infection, therefore, accounts for the reduction of PHN [36] . One approach to the prevention of PHN in those who already harboring VZV involves the administration of the Varicella zoster vaccine (Zostavax), which has been approved by the FAD above 50 years [32] . The Zostavax vaccine, which activates specific T-cell production and thus prevents viral reactivations, was found to be effective in reducing the burden of illness due to HZ, incidence of HZ, and incidence of PHN. Therefore, zoster vaccination reduced overall HZ and PHN incidence by 51.3% and 66.5%, respectively [37] . However, despite the promising results of immunization, the vaccine remains widely underused, mainly due to the lack of recommendation by physicians and dermatologists as well as lack of awareness of disease. According to “The Centers for Disease Control and Prevention”, recommends one dose of the HZ vaccine should be given above 60 years age [38] . Vaccine is contraindicated in patients with blood cancer, pregnancy and acquired immune deficiency syndrome (AIDS).
The role of antiviral drugs (acyclovir, famciclovir, and valacyclovir) in PHN prevention is still controversial. In spite of that, studies done by different physicians with different designs suggest that antiviral drugs can slow the production of the virus and decreases the viral load in the dorsal root ganglia. These agents reduce the duration of viral shedding, hasten rash healing, reduce the severity and duration of acute pain, and reduce the risk of progression to PHN [39] . For example, Dworkin et al. [40] and Parruti et al. [41] done a cohort study of 419 and 519 Hz patients respectively found that patients receiving antiviral therapy in the acute phase had a significantly lower prevalence of PHN.
4. Summary and Prospective
PHN is one of the most common and intractable neuropathic pain disorders of HZ which often accompanied by physical, social, psychological and occupational disorder. Optimal management of pain in PHN patients is complex and difficult. There are several therapeutic options to treat PHN but better utilization of available options to PHN management is based on the patient’s individual characteristics. According to FDA protocol the use of anticonvulsants, TCAs and a 5% lidocaine patch is the first line treatments and Opioids/topical capsaicin patch or cream is the second-line treatments for PHN. The main therapies for prevention of PHN include vaccination and antiviral therapy in acute phase. Population-based programs for vaccination of elderly and possibly younger adults for HZ appear at present the best preventive approach. Timely antiviral treatment of HZ may likely be another tool for prevention, especially for those patients with multiple attack of PHN at the onset of HZ. Education for both the health care providers and the patients and their families is the most important step in the prevention of PHN.
This review also recalls the attention of all dermatologists to know that ozone therapy is a most valuable tool for the medical treatment of PHN in reducing the pain. At last PHN remains a potentially debilitating and undertreated form of neuropathic pain. Over the past decade, clinical findings and treatment guidelines have underscored the importance of increased clinician awareness of the signs and symptoms of this chronically painful disorder and the importance of deploying evidence-based treatment modalities to improve outcome. This review will help to understand the latest drugs and technology for the treatment and prevention of PHN.
Conflict of Interest
We declare that none of the authors have any financial and personal relationships with other people or organizations that can inappropriately influence the quality of the work presented in this manuscript. There is no professional or other personal interest of any nature or kind in any product, service and/or company that could be construed as influencing the position presented in, or the review of, the manuscript entitled, “The Current Treatment and Prevention of Post Herpetic Neuralgia”.
Acknowledgements
This research is supported by the National Natural Science Foundation of China (31700736), Hubei Province Natural Science Foundation of China (2016CFB180) and Hubei Province Health and Family Planning Scientific Research Project (WJ2016Y07).
Cite this paper
Ankit, S., Zeng, T.X., Chen, Y.X., Gupta, H.N., Shah, K. and Wang, X.W. (2018) The Current Treatment and Prevention of Post Herpetic Neuralgia. Yangtze Medicine, 2, 28-38. https://doi.org/10.4236/ym.2018.21003
References
- 1. Wollina, U. and Machetanz, J. (2016) Herpes Zoster and Postherpetic Neuralgia. Hautarzt, 67, 653-665. https://doi.org/10.1007/s00105-016-3834-y
- 2. Ansar, A., et al. (2014) Association between Family History and Herpes Zoster: A Case-Control Study. Journal of Research in Health Sciences, 14, 111-114.
- 3. Portenoy, R.K., Duma, C. and Foley, K.M. (1986) Acute Herpetic and Postherpetic Neuralgia: Clinical Review and Current Management. Annals of Neurology, 20, 651-664. https://doi.org/10.1002/ana.410200602
- 4. Dworkin, R.H., et al. (2008) Diagnosis and Assessment of Pain Associated with Herpes Zoster and Postherpetic Neuralgia. Journal of Pain, 9, S37-S44. https://doi.org/10.1016/j.jpain.2007.10.008
- 5. Drolet, M., et al. (2010) Predictors of Postherpetic Neuralgia among Patients with Herpes Zoster: A Prospective Study. Journal of Pain, 11, 1211-1221. https://doi.org/10.1016/j.jpain.2010.02.020
- 6. High, K.P. (2007) Preventing Herpes Zoster and Postherpetic Neuralgia through Vaccination. The Journal of Family Practice, 56, 51A-57A.
- 7. Stein, A.N., et al. (2009) Herpes Zoster Burden of Illness and Health Care Resource Utilisation in the Australian Population Aged 50 Years and Older. Vaccine, 27, 520-529. https://doi.org/10.1016/j.vaccine.2008.11.012
- 8. Johnson, B.H., et al. (2015) Annual Incidence Rates of Herpes Zoster among an Immunocompetent Population in the United States. BMC Infectious Diseases, 15, 502. https://doi.org/10.1186/s12879-015-1262-8
- 9. Choi, W.S., et al. (2010) Disease Burden of Herpes Zoster in Korea. Journal of Clinical Virology, 47, 325-329. https://doi.org/10.1016/j.jcv.2010.01.003
- 10. Li, Y., et al. (2016) Disease Burden Due to Herpes Zoster among Population Aged >/=50 Years Old in China: A Community Based Retrospective Survey. PLoS One, 11, e0152660. https://doi.org/10.1371/journal.pone.0152660
- 11. Argoff, C.E. (2011) Review of Current Guidelines on the Care of Postherpetic Neuralgia. Postgraduate Medical Journal, 123, 134-142. https://doi.org/10.3810/pgm.2011.09.2469
- 12. Nalamachu, S. and Morley-Forster, P. (2012) Diagnosing and Managing Postherpetic Neuralgia. Drugs Aging, 29, 863-869. https://doi.org/10.1007/s40266-012-0014-3
- 13. Baron, R. (2009) Neuropathic Pain: A Clinical Perspective. Handbook of Experimental Pharmacology, 194, 3-30. https://doi.org/10.1007/978-3-540-79090-7_1
- 14. Singh, S., et al. (2013) Post-Herpetic Neuralgia: A Review of Current Management Strategies. Indian Journal of Pain, 27, 12-21. https://doi.org/10.4103/0970-5333.114857
- 15. Gupta, R., et al. (2013) Post-Herpetic Neuralgia: A Review of Current Management Strategies. Indian Journal of Pain, 27, 12. https://doi.org/10.4103/0970-5333.114857
- 16. Rowbotham, M.C., et al. (1996) Lidocaine Patch: Double-Blind Controlled Study of a New Treatment Method for Post-Herpetic Neuralgia. Pain, 65, 39-44. https://doi.org/10.1016/0304-3959(95)00146-8
- 17. Harden, R.N., et al. (2013) Evidence-Based Guidance for the Management of Postherpetic Neuralgia in Primary Care. Postgraduate Medicine, 125, 191-202. https://doi.org/10.3810/pgm.2013.07.2690
- 18. Watson, P.N. (2010) Postherpetic Neuralgia. BMJ Clinical Evidence, 2010, Article ID: 0905.
- 19. Khaliq, W., Alam, S. and Puri, N.K. (2013) Withdrawn: Topical Lidocaine for the Treatment of Postherpetic Neuralgia. The Cochrane Database of Systematic Reviews, No. 10, Cd004846.
- 20. Ballantyne, J.C. and Mao, J. (2003) Opioid Therapy for Chronic Pain. The New England Journal of Medicine, 349, 1943-1953. https://doi.org/10.1056/NEJMra025411
- 21. Eisenberg, E., McNicol, E.D. and Carr, D.B. (2005) Efficacy and Safety of Opioid Agonists in the Treatment of Neuropathic Pain of Nonmalignant Origin: Systematic Review and Meta-Analysis of Randomized Controlled Trials. JAMA, 293, 3043-3052. https://doi.org/10.1001/jama.293.24.3043
- 22. Gavin, P.D., et al. (2017) Transdermal Oxycodone Patch for the Treatment of Postherpetic Neuralgia: A Randomized, Double-Blind, Controlled Trial. Pain Management, 7, 255-267. https://doi.org/10.2217/pmt-2016-0067
- 23. Zin, C.S., et al. (2010) A Randomized, Controlled Trial of Oxycodone versus Placebo in Patients with Postherpetic Neuralgia and Painful Diabetic Neuropathy Treated with Pregabalin. Journal of Pain, 11, 462-471. https://doi.org/10.1016/j.jpain.2009.09.003
- 24. Dubinsky, R.M., et al. (2004) Practice Parameter: Treatment of Postherpetic Neuralgia: An Evidence-Based Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology, 63, 959-965. https://doi.org/10.1212/01.WNL.0000140708.62856.72
- 25. Whitley, R.J., et al. (1996) Acyclovir with and without Prednisone for the Treatment of Herpes Zoster. A Randomized, Placebo-Controlled Trial. Annals of Internal Medicine, 125, 376-383. https://doi.org/10.7326/0003-4819-125-5-199609010-00004
- 26. Saarto, T. and Wiffen, P.J. (2010) Antidepressants for Neuropathic Pain: A Cochrane Review. Journal of Neurology, Neurosurgery, and Psychiatry, 81, 1372-1373. https://doi.org/10.1136/jnnp.2008.144964
- 27. Pasqualucci, A., et al. (2000) Prevention of Post-Herpetic Neuralgia: Acyclovir and Prednisolone versus Epidural Local Anesthetic and Methylprednisolone. Acta Anaesthesiologica Scandinavica, 44, 910-918. https://doi.org/10.1034/j.1399-6576.2000.440803.x
- 28. Makharita, M.Y., Amr, Y.M. and El-Bayoumy, Y. (2015) Single Paravertebral Injection for Acute Thoracic Herpes Zoster: A Randomized Controlled Trial. Pain Practice, 15, 229-235. https://doi.org/10.1111/papr.12179
- 29. Ji, G., et al. (2009) The Effectiveness of Repetitive Paravertebral Injections with Local Anesthetics and Steroids for the Prevention of Postherpetic Neuralgia in Patients with Acute Herpes Zoster. Anesthesia & Analgesia, 109, 1651-1655. https://doi.org/10.1213/ANE.0b013e3181b79075
- 30. Makharita, M.Y., Amr, Y.M. and El-Bayoumy, Y. (2012) Effect of Early Stellate Ganglion Blockade for Facial Pain from Acute Herpes Zoster and Incidence of Postherpetic Neuralgia. Pain Physician, 15, 467-474.
- 31. Mallick-Searle, T., Snodgrass, B. and Brant, J.M. (2016) Postherpetic Neuralgia: Epidemiology, Pathophysiology, and Pain Management Pharmacology. Journal of Multidisciplinary Healthcare, 9, 447-454. https://doi.org/10.2147/JMDH.S106340
- 32. Massengill, J.S. and Kittredge, J.L. (2014) Practical Considerations in the Pharmacological Treatment of Postherpetic Neuralgia for the Primary Care Provider. Journal of Pain Research, 7, 125-132. https://doi.org/10.2147/JPR.S57242
- 33. Sampathkumar, P., Drage, L.A. and Martin, D.P. (2009) Herpes Zoster (Shingles) and Postherpetic Neuralgia. Mayo Clinic Proceedings, 84, 274-280. https://doi.org/10.4065/84.3.274
- 34. Konrad, D.H. (1981) Ozone Therapy for Post-Herpetic Neuralgia. Largo Como, Säo Paulo.
- 35. Luo, W.J., et al. (2017) Intervertebral Foramen Injection of Ozone Relieves Mechanical Allodynia and Enhances Analgesic Effect of Gabapentin in Animal Model of Neuropathic Pain. Pain Physician, 20, E673-E685.
- 36. Goldman, G.S. and King, P.G. (2013) Review of the United States Universal Varicella Vaccination Program: Herpes Zoster Incidence Rates, Cost-Effectiveness, and Vaccine Efficacy Based Primarily on the Antelope Valley Varicella Active Surveillance Project Data. Vaccine, 31, 1680-1694. https://doi.org/10.1016/j.vaccine.2012.05.050
- 37. Oxman, M.N., et al. (2005) A Vaccine to Prevent Herpes Zoster and Postherpetic Neuralgia in Older Adults. The New England Journal of Medicine, 352, 2271-2284. https://doi.org/10.1056/NEJMoa051016
- 38. Makharita, M.Y. (2017) Prevention of Post-Herpetic Neuralgia from Dream to Reality: A Ten-Step Model. Pain Physician, 20, E209-E220.
- 39. Fashner, J. and Bell, A.L. (2011) Herpes Zoster and Postherpetic Neuralgia: Prevention and Management. American Family Physician, 83, 1432-1437.
- 40. Dworkin, R.H., et al. (1998) Postherpetic Neuralgia: Impact of Famciclovir, Age, Rash Severity, and Acute Pain in Herpes Zoster Patients. The Journal of Infectious Diseases, 178, S76-S80. https://doi.org/10.1086/514260
- 41. Parruti, G., et al. (2010) Predictors of Pain Intensity and Persistence in a Prospective Italian Cohort of Patients with Herpes Zoster: Relevance of Smoking, Trauma and Antiviral Therapy. BMC Medicine, 8, 58-67. https://doi.org/10.1186/1741-7015-8-58
Abbreviation
PHN: Post Herpetic Neuralgia
HZ: Herpes Zoster
NDA: New Drug Application
PPAR: Peroxisome Proliferator Activator Receptor
FDA: Food and Drug Administration
TRPV1: Transient Receptor Potential Vanilloid 1 Receptor
PVB: Para Vertebral Block
IV: Intravenous
上一篇:Nursing Students’ Experience 下一篇:The Influence of Gastrodin on
最新文章NEWS
- Prevention of Nephropathy by Some Natural Sources of Antioxidants
- Molecular Motors—Self-Organization of Cytoskeletal Network
- Effects of 72 Hours Sleep Deprivation on Liver Circadian Clock Gene Expression and Oxidative Stress
- A Case of Refractory Insomnia Responding to Modified Electroconvulsive Therapy
- Prevalence of Coinfection with Malaria and HIV among Children in Yaoundé, Cameroon: A Cross-Sectiona
- Logistic Regression Analysis the Risk Factors of Peripherally Inserted Central Catheter Related Bloo
- Nursing Students’ Experience with Information Literacy Skill
- Colorectal Adenocarcinoma Post-Operative Treatment with Chinese Herbs
推荐期刊Tui Jian
- Chinese Journal of Integrative Medicine
- Journal of Genetics and Genomics
- Journal of Bionic Engineering
- Pedosphere
- Chinese Journal of Structural Chemistry
- Nuclear Science and Techniques
- 《传媒》
- 《中学生报》教研周刊
热点文章HOT
- Development and Validation of an LC-MS/MS Method for Determination of Catalpol and Harpagide in Smal
- Microarray Analysis of microRNAs Expression Profiles in Adult and Aged Mice Hippocampus
- Prevention of Nephropathy by Some Natural Sources of Antioxidants
- Prevalence of Coinfection with Malaria and HIV among Children in Yaoundé, Cameroon: A Cross-Sectiona
- The Influence of Gastrodin on Expression of IL-10, STAT3 and JAK2 in Epileptic Rats’ Hippocampus
- Carbonic Anhydrase III S-Glutathionylation Is Necessary for Anti-Oxidant Activity
- Hyaluronic Acid in the Treatment of Knee Osteoarthritis: Review
- Molecular Motors—Self-Organization of Cytoskeletal Network